
The healthcare industry is increasingly reliant on electronic medical records (EMRs) and digital documentation. One of the most crucial components of this digital transformation is the Soap Note Template Word, a standardized format for capturing patient information and clinical notes. This article will delve into the purpose, benefits, creation, and best practices for utilizing a robust Soap Note Template Word to streamline workflows, improve patient care, and enhance data analysis. Understanding the nuances of this template is vital for clinicians, nurses, and healthcare administrators alike. The core function of a well-structured Soap Note Template Word is to provide a clear, concise, and easily accessible record of a patient’s encounter, facilitating seamless communication between providers and ensuring continuity of care. It’s more than just a document; it’s a vital tool for quality improvement and operational efficiency.
What is a Soap Note Template Word?
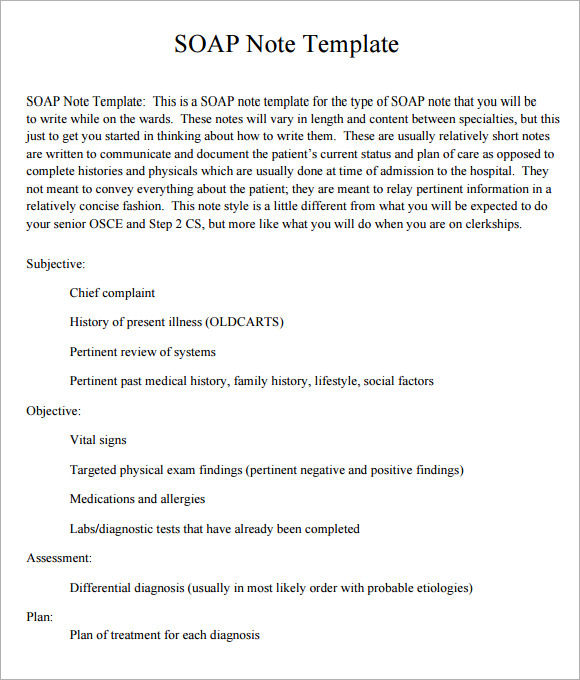
A Soap Note Template Word is a standardized, digital format designed to capture essential patient information during a clinical encounter. It’s a structured document that guides clinicians in documenting their observations, assessments, and interventions. Unlike free-form notes, a Soap Note Template Word enforces a consistent structure, promoting clarity, accuracy, and ease of retrieval. It’s not just a collection of notes; it’s a framework built around specific elements designed to facilitate efficient communication and data management. The template typically includes sections for demographics, chief complaint, history of present illness (HPI), physical exam findings, assessment, plan, and follow-up instructions. The goal is to create a readily accessible and easily searchable record of the patient’s experience. Different healthcare organizations and facilities may have slightly varying versions of the template, but the core principles remain consistent.

The Benefits of Using a Soap Note Template Word
Implementing a standardized Soap Note Template Word offers a multitude of benefits across various aspects of healthcare. Firstly, it significantly improves documentation accuracy and reduces the risk of errors. The structured format minimizes the potential for omissions or misinterpretations, leading to more reliable patient records. Secondly, it streamlines workflows, reducing the time spent on note-taking and facilitating faster transitions between providers. This is particularly beneficial in busy clinical settings. Thirdly, the standardized format enhances data analysis and facilitates population health management. By consistently capturing relevant information, the template enables healthcare providers to identify trends, track patient outcomes, and evaluate the effectiveness of interventions. Furthermore, it supports electronic health record (EHR) integration by providing a consistent interface for data exchange between different systems. Finally, the use of a Soap Note Template Word contributes to improved patient safety by ensuring that all relevant information is captured and readily available to authorized personnel.

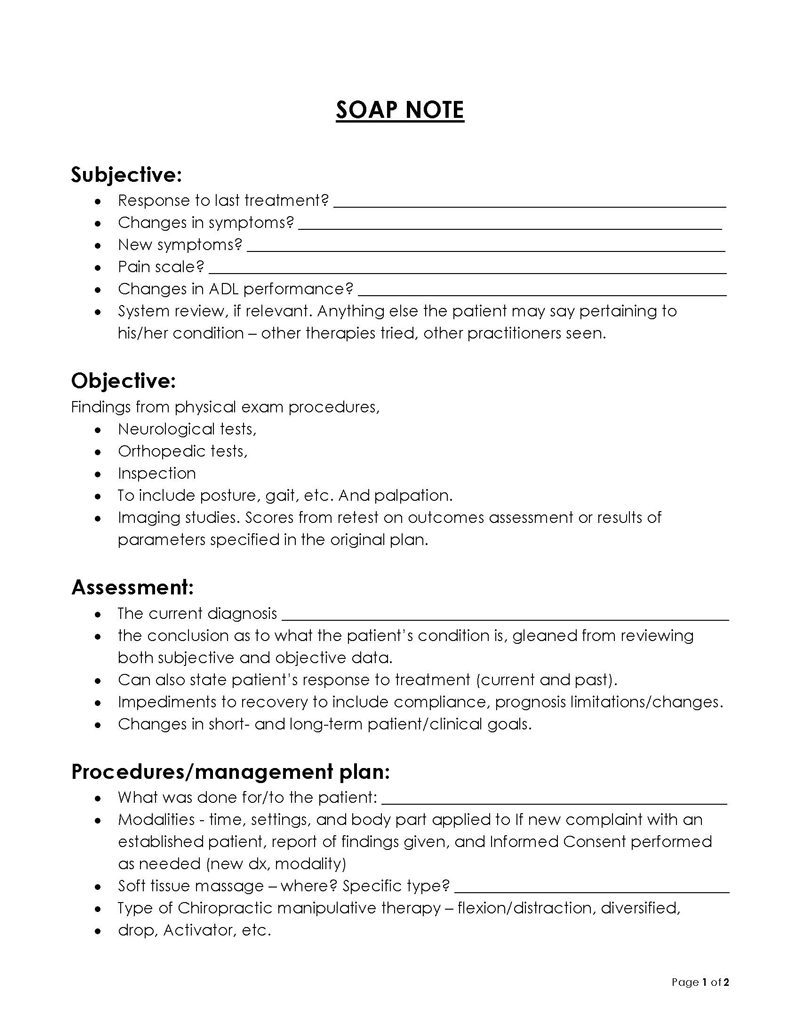
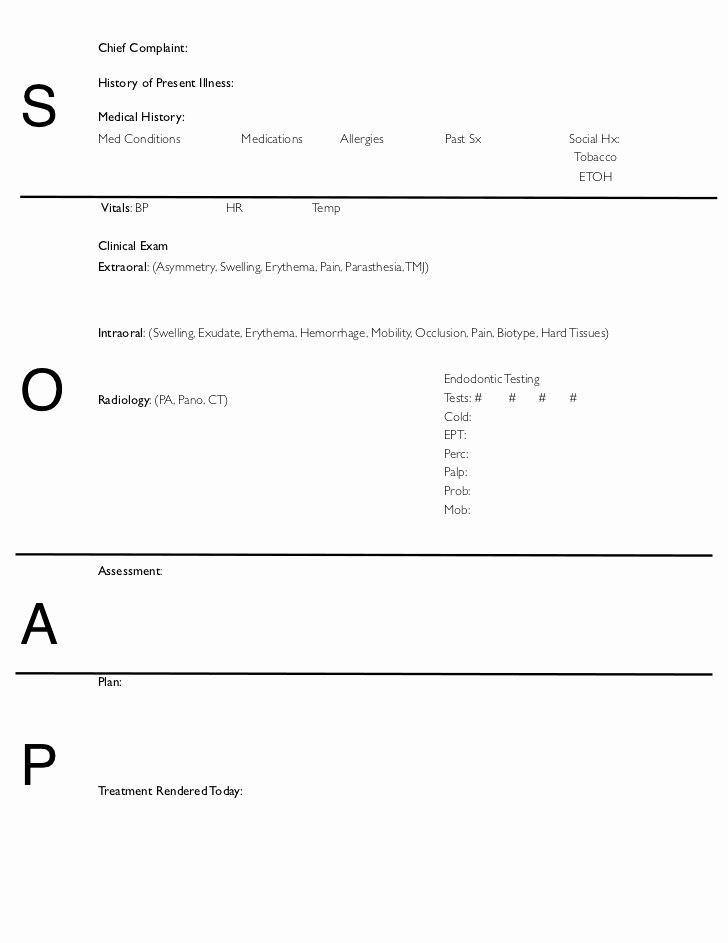
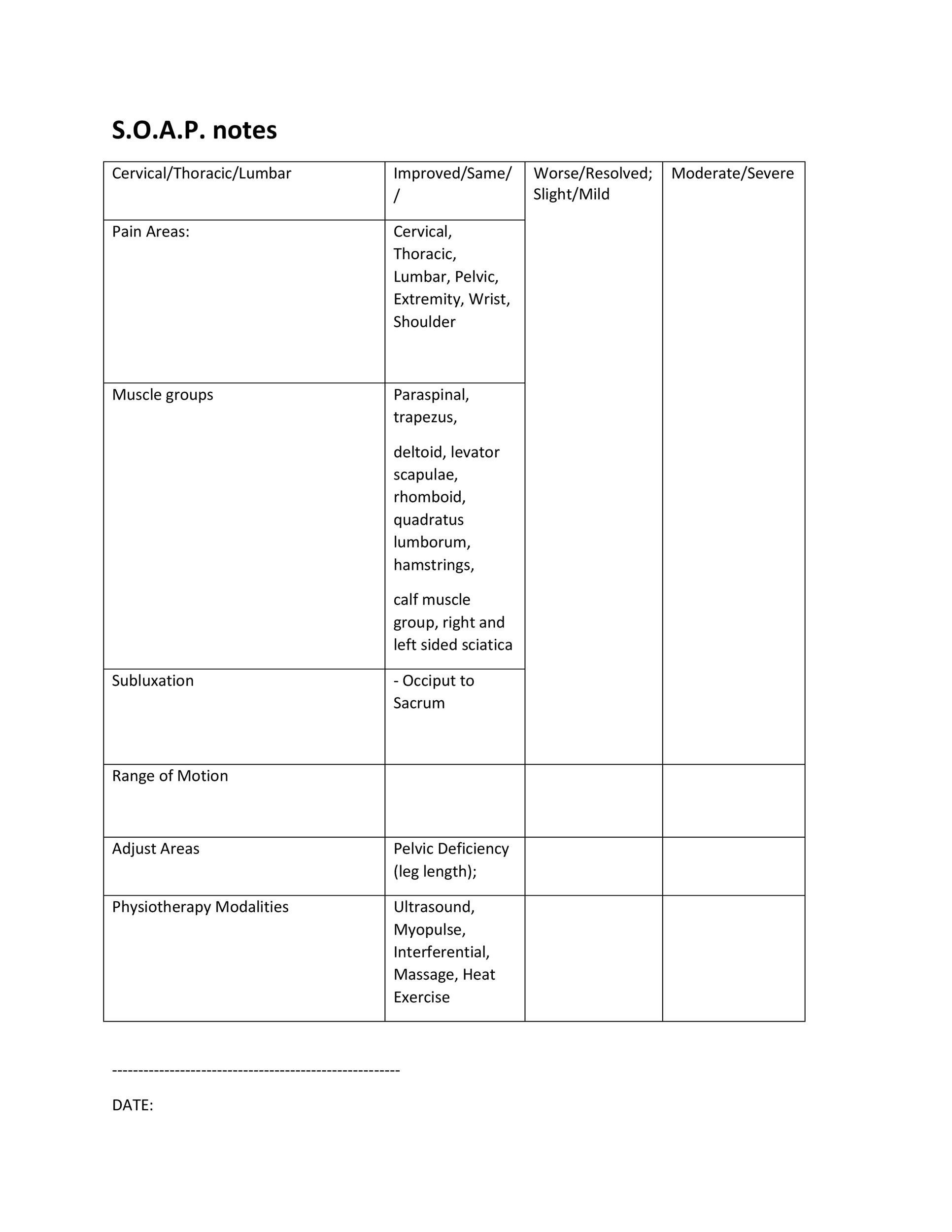
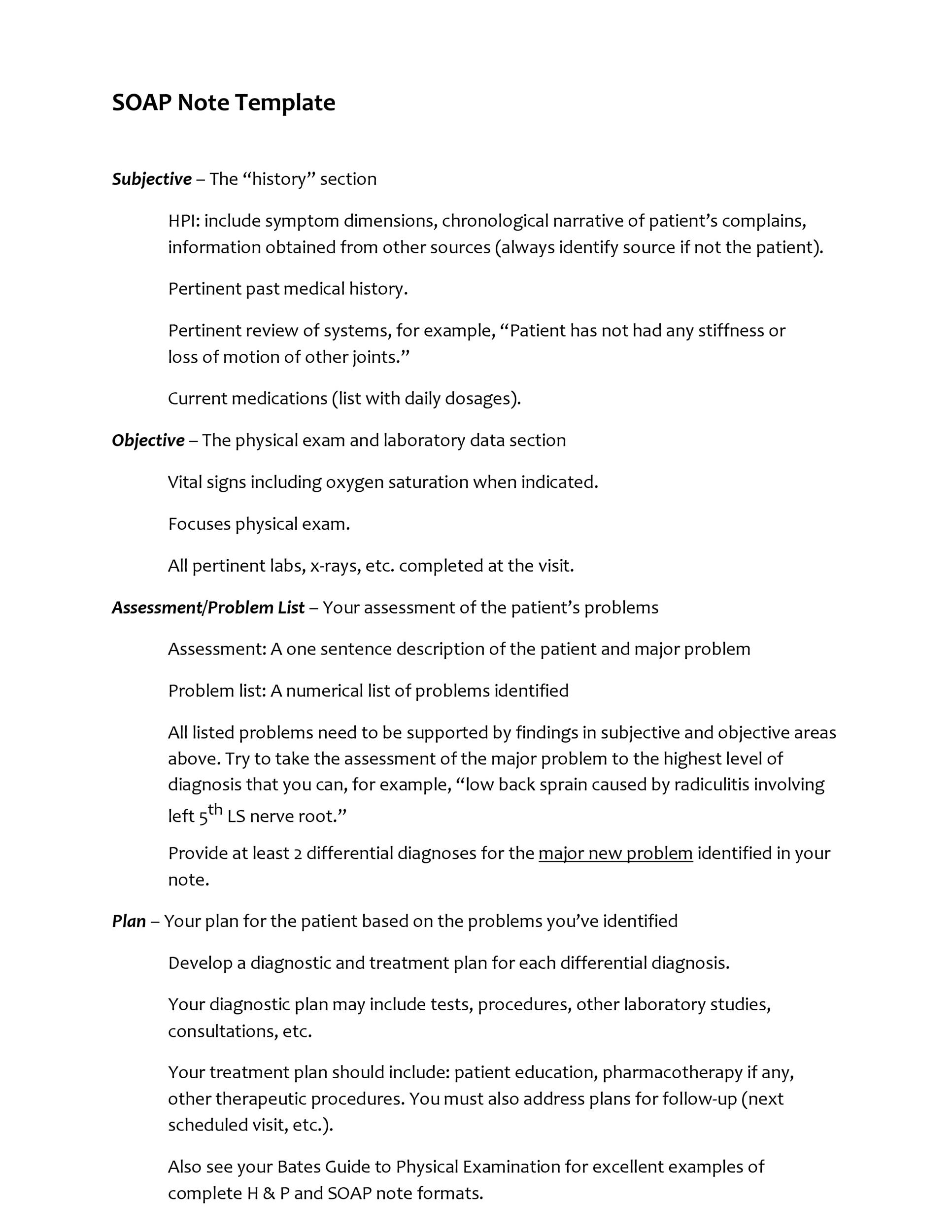
Key Sections of a Standardized Soap Note Template Word
Let’s examine some of the key sections commonly found within a typical Soap Note Template Word. Each section is designed to capture specific aspects of the patient encounter.
1. Patient Demographics
This section gathers essential information about the patient, including:
- Patient Name: Full name, including any nicknames.
- Date of Birth: Crucial for accurate record-keeping.
- Medical Record Number (MRN): Unique identifier for the patient.
- Contact Information: Phone number, address, and emergency contact details.
- Insurance Information: Policy number and group name.
2. Chief Complaint
This section clearly states the patient’s primary reason for seeking medical attention. It’s a concise and easily understandable summary of the patient’s main concern.
- Chief Complaint: A brief, one-sentence description of the patient’s problem. Example: “Chest pain.”
3. History of Present Illness (HPI)
This section provides a detailed account of the patient’s current condition, including:
- Onset: When did the symptoms begin?
- Location: Where are the symptoms located?
- Character: What does the symptom feel like (e.g., sharp, dull, throbbing)?
- Radiation: Does the symptom spread to other areas?
- Timing: How long does the symptom last?
- Aggravating Factors: What makes the symptom worse?
- Relieving Factors: What makes the symptom better?
- Severity: How severe is the symptom (e.g., mild, moderate, severe)?
4. Past Medical History (PMH)
This section outlines the patient’s previous medical conditions, surgeries, hospitalizations, and allergies.

- Past Medical Conditions: List of chronic diseases, surgeries, and hospitalizations.
- Allergies: List of medications, food, and environmental allergies.
- Immunizations: Vaccination history.
5. Medications
This section details the patient’s current medications, including dosage, frequency, and route of administration.

- Current Medications: List of all medications, including generic and brand names.
- Prescription Medications: List of current prescriptions.
- Over-the-Counter Medications: List of OTC medications.
6. Social History
This section covers the patient’s lifestyle factors, including:
- Smoking Status: Current smoker, former smoker, never smoked.
- Alcohol Use: Frequency and amount of alcohol consumption.
- Drug Use: History of illicit drug use.
- Occupation: Patient’s job or profession.
- Living Situation: Living situation (e.g., alone, with family, assisted living).
7. Physical Examination
This section describes the findings from the physical examination, including:
- Vital Signs: Temperature, blood pressure, heart rate, respiratory rate, and oxygen saturation.
- General Appearance: Patient’s overall appearance and demeanor.
- Head-to-Toe Examination: Findings from examining different body systems.
- Specific Findings: Detailed descriptions of any abnormalities observed.
8. Assessment
This section summarizes the provider’s assessment of the patient’s condition, including:
- Diagnosis: The patient’s primary diagnosis.
- Differential Diagnosis: Other possible diagnoses considered.
- Problem List: A list of the patient’s key problems.
9. Plan
This section outlines the proposed treatment plan, including:
- Treatment Recommendations: Specific recommendations for treatment.
- Medications: Prescription medications, dosages, and instructions.
- Lifestyle Modifications: Recommendations for lifestyle changes (e.g., diet, exercise).
- Follow-up Instructions: Instructions for follow-up appointments and testing.
10. Follow-up Instructions
This section provides instructions for the patient and provider regarding the next steps.
- Follow-up Appointment: Date and time of the next appointment.
- Testing: Instructions for any required tests.
- Contact Information: Contact information for the patient and provider.
The Importance of Standardization
The consistent application of a Soap Note Template Word is paramount for several reasons. It ensures that all providers are documenting the same information, reducing the risk of errors and inconsistencies. It facilitates communication between providers, allowing them to share information seamlessly. Furthermore, the standardized format makes it easier to track patient outcomes and identify areas for improvement. Regular audits and quality assurance programs are essential to maintain the integrity of the Soap Note Template Word and ensure its continued effectiveness.
Conclusion
The Soap Note Template Word represents a significant advancement in healthcare documentation. By providing a structured and standardized framework, it streamlines workflows, improves patient care, and enhances data management. While variations exist across different organizations, the core principles of clarity, accuracy, and consistency remain essential. As healthcare technology continues to evolve, the Soap Note Template Word will undoubtedly remain a cornerstone of efficient and effective patient care. Investing in the proper training and implementation of this template is a strategic investment in the overall quality of healthcare delivery. The benefits, from reduced errors to improved patient outcomes, are substantial and justify the effort involved in adopting and maintaining a robust Soap Note Template Word system.