Physical therapy (PT) documentation is a critical component of effective patient care. Accurate, comprehensive, and well-organized documentation ensures seamless communication between therapists, physicians, and other healthcare professionals, ultimately leading to improved patient outcomes. Physical Therapy Documentation Templates are designed to streamline this process, providing a standardized framework for recording patient information, treatment plans, and progress reports. They are not just about paperwork; they’re about ensuring clarity, accountability, and efficient workflow. Choosing the right template can significantly reduce errors, improve documentation quality, and save valuable time. This article will explore the key elements of effective physical therapy documentation templates, offering practical guidance and best practices for practitioners.
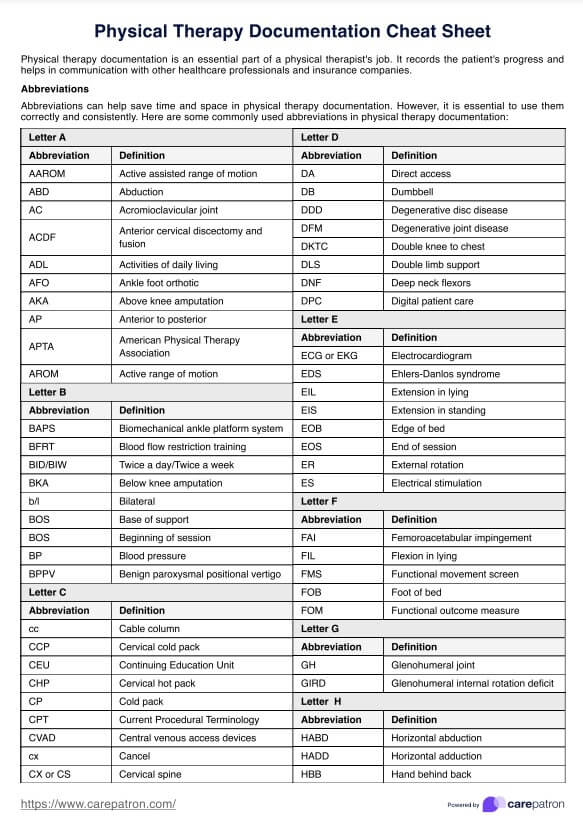
Understanding the Importance of Documentation
The initial stages of a physical therapy session often involve a thorough assessment. Detailed documentation of this assessment – including patient history, current condition, limitations, and goals – is paramount. Without this information, it’s difficult to tailor the treatment plan to the individual patient’s needs. Furthermore, documentation serves as a record of the therapy provided, allowing for retrospective analysis of treatment effectiveness and identifying areas for improvement. Poorly documented sessions can lead to misunderstandings, duplicated efforts, and ultimately, suboptimal patient care. Investing in robust documentation practices is, therefore, a vital investment in the quality of physical therapy. The ability to accurately and comprehensively document a patient’s journey is a cornerstone of their rehabilitation.
.png)
Key Components of a Physical Therapy Documentation Template
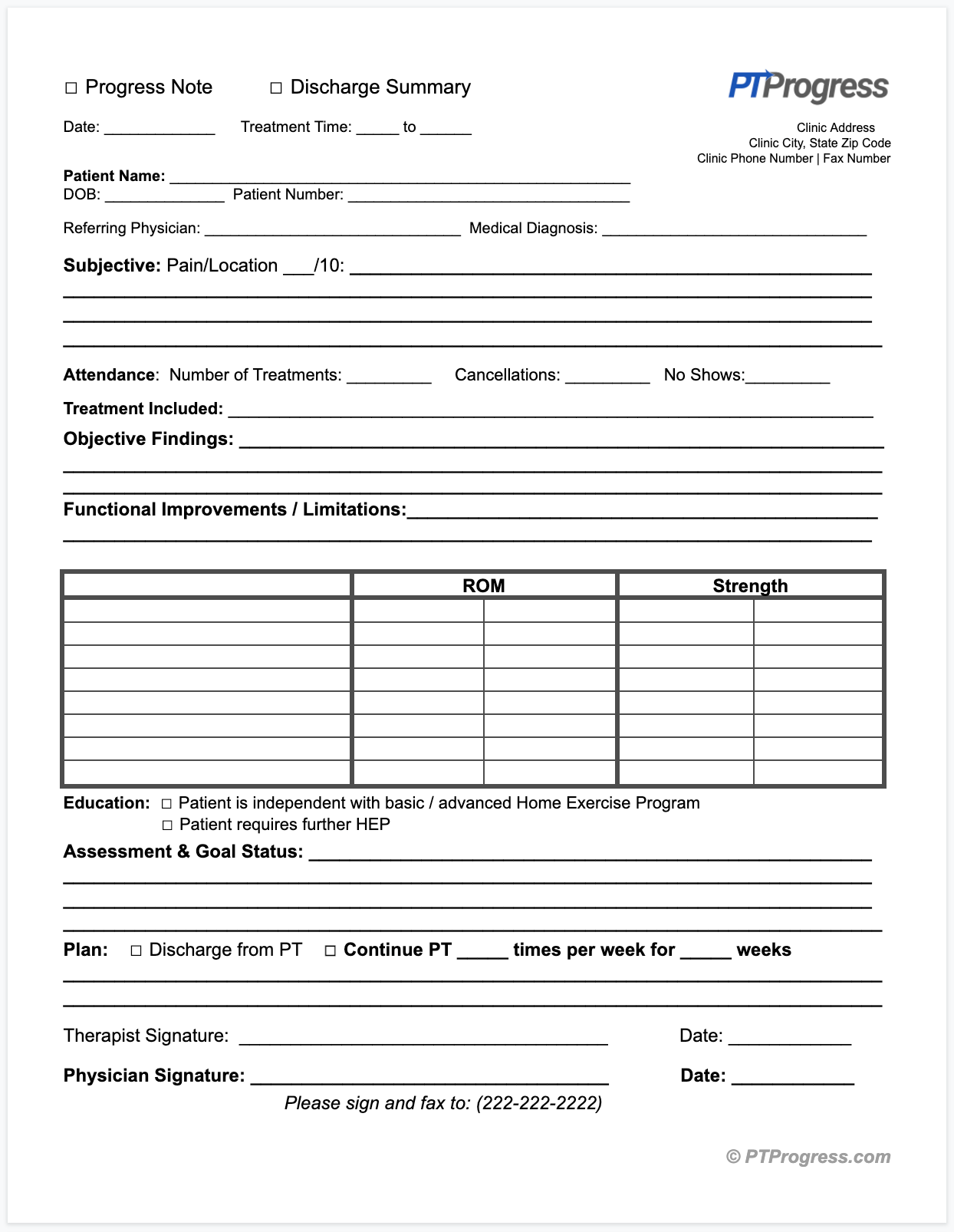
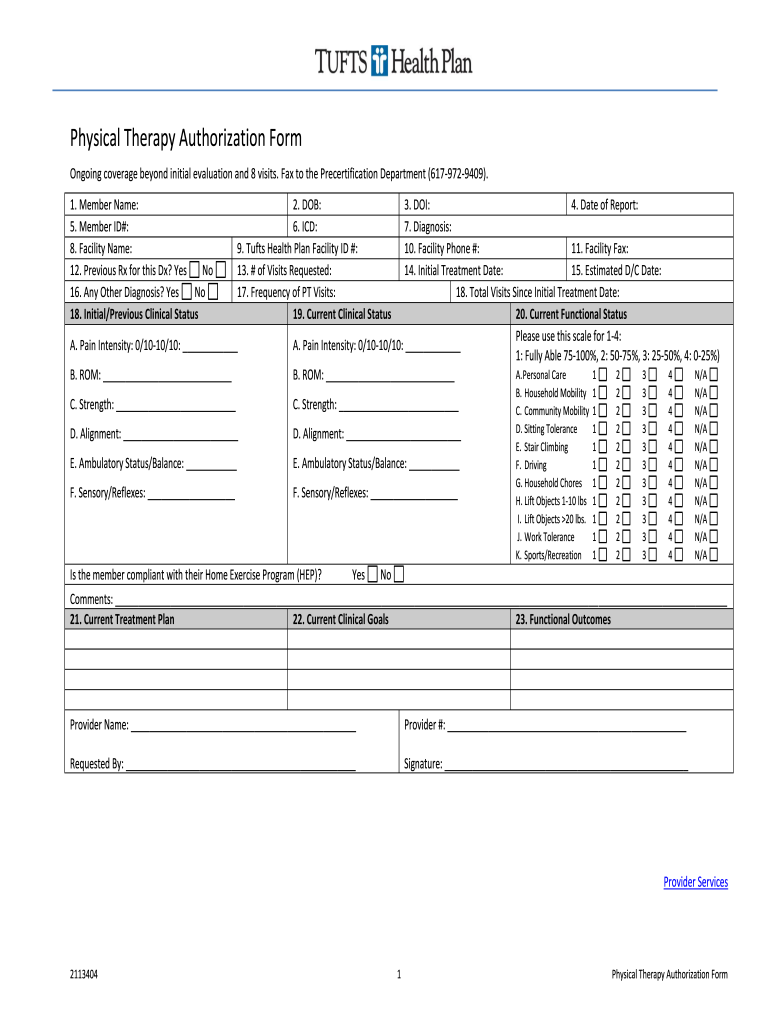
A well-structured physical therapy documentation template typically includes several key sections. Each section is designed to gather specific information relevant to the patient’s condition and treatment plan. Here’s a breakdown of the essential elements:
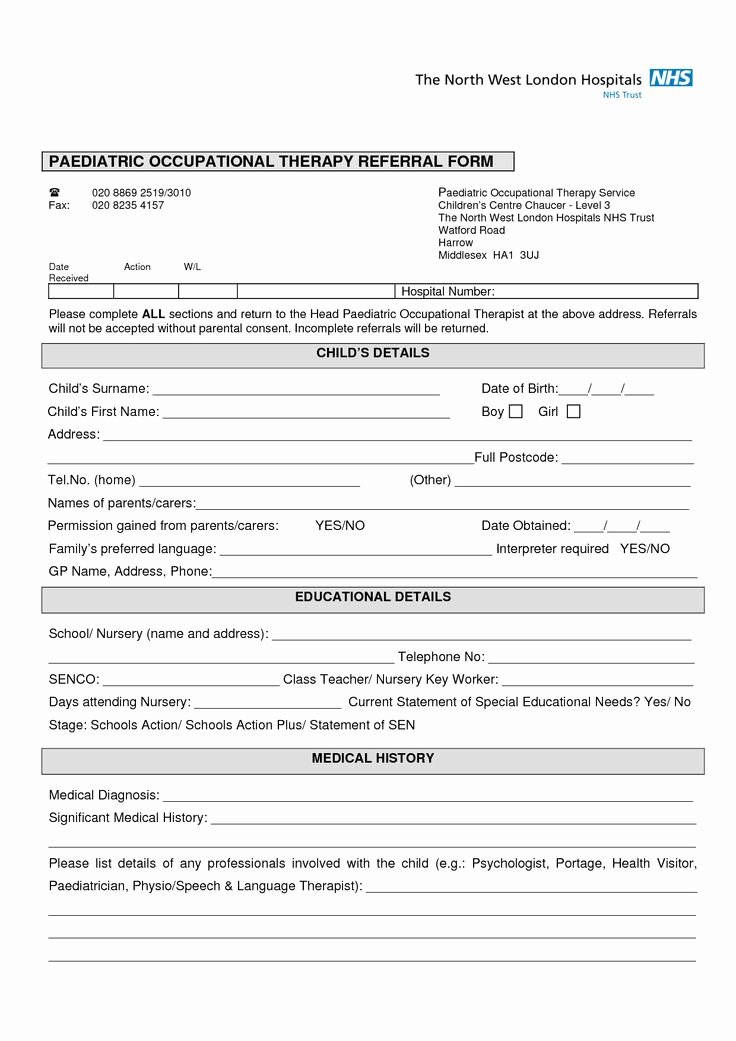
1. Patient Demographics & Contact Information
This section provides basic information about the patient, ensuring easy identification and tracking. It includes:
- Patient Name: Full name, preferred name.
- Date of Birth: Essential for accurate record-keeping.
- Contact Information: Phone number, email address.
- Insurance Information: Policy number, group number.
- Referring Physician: Name and contact information of the physician providing the care.
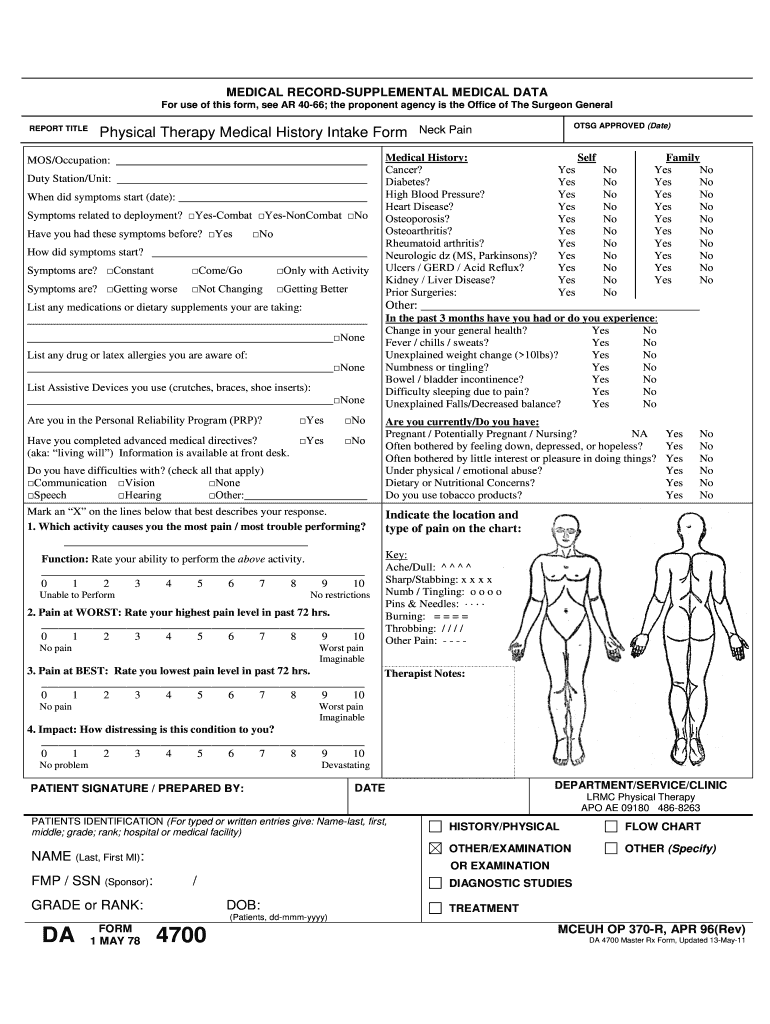
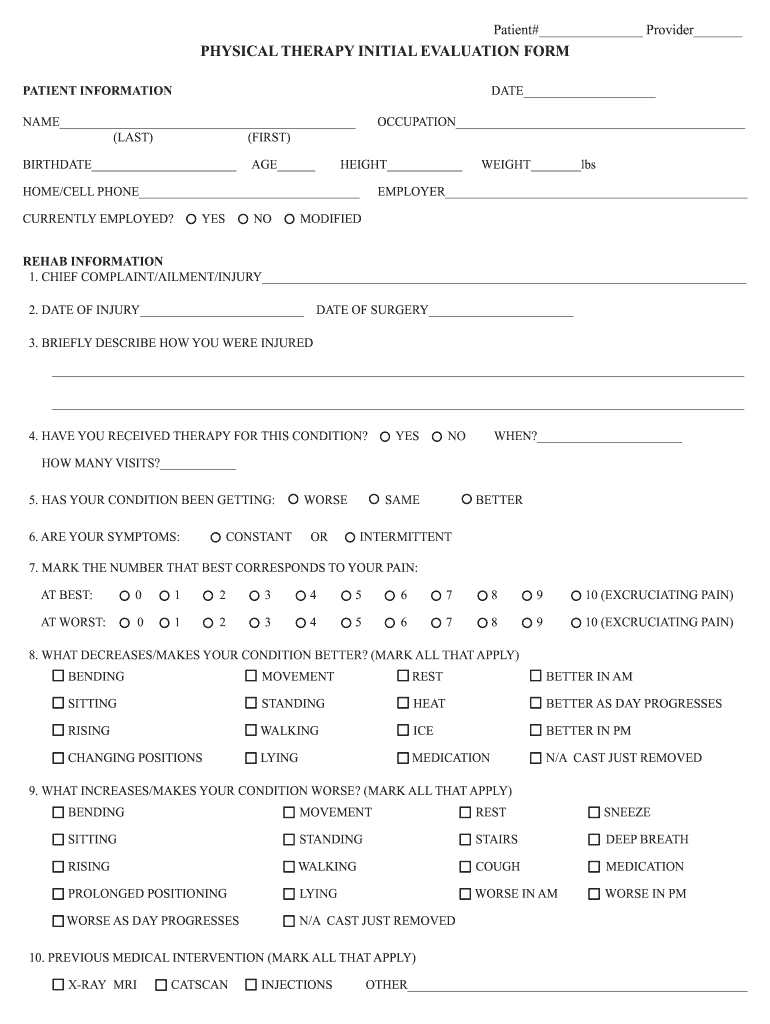
2. Initial Assessment
This section captures the patient’s initial condition upon admission or initial visit. It should include:

- Chief Complaint: The patient’s primary reason for seeking physical therapy.
- History of Present Illness (HPI): A detailed description of the patient’s current problem, including onset, duration, severity, and aggravating/alleviating factors.
- Past Medical History: Relevant medical conditions, surgeries, and medications.
- Social History: Information about the patient’s lifestyle, including occupation, activity level, and support system.
- Physical Examination Findings: A comprehensive description of the patient’s physical condition, including range of motion, strength, posture, and functional limitations. This section should be detailed and objective.
3. Treatment Plan
This is arguably the most crucial section, outlining the specific interventions planned for the patient. It should include:
- Treatment Goals: Clearly defined, measurable, achievable, relevant, and time-bound (SMART) goals.
- Treatment Modalities: Specific techniques and exercises to be used (e.g., range of motion exercises, strengthening exercises, manual therapy, modalities).
- Treatment Frequency & Duration: How often and for how long each intervention will be performed.
- Patient Education: Information provided to the patient regarding their condition, treatment plan, and self-care strategies.
- Progress Notes: Regular updates on the patient’s progress, including observed improvements, challenges, and any changes to the treatment plan.
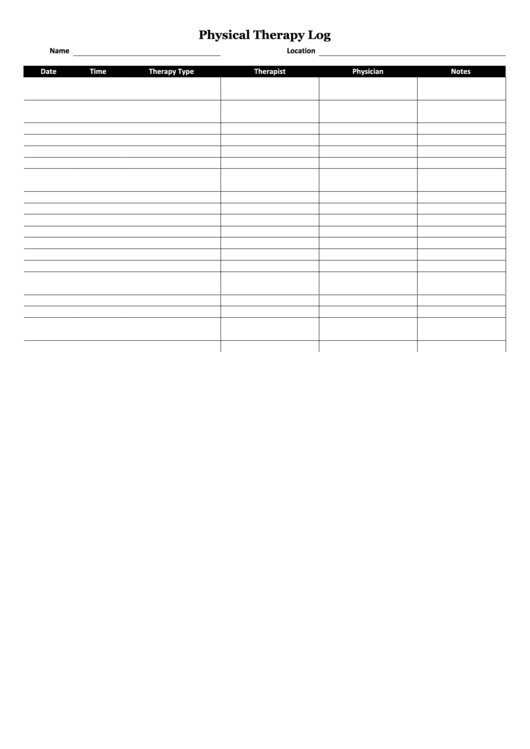
4. Progress Notes
Detailed notes are essential for tracking the patient’s response to treatment. These notes should be concise, objective, and focused on the patient’s functional progress. They should include:
- Date and Time of Assessment
- Specific Observations: Describe what the therapist observed during the assessment.
- Patient Response: Document the patient’s reaction to the treatment (e.g., improvement, stabilization, worsening).
- Functional Improvements: Quantify any changes in the patient’s ability to perform specific tasks (e.g., walking distance, lifting capacity, balance).
- Challenges Encountered: Document any difficulties the patient experienced during treatment.
Utilizing Templates Effectively: Best Practices
While templates provide a solid foundation, tailoring them to the individual patient’s needs is key. Consider these best practices:
- Use Clear and Concise Language: Avoid jargon and technical terms that the patient may not understand.
- Be Objective: Focus on observable data rather than subjective opinions.
- Include Visual Aids: Supplement written notes with photographs or diagrams to illustrate treatment plans and patient progress.
- Regularly Review and Update: Templates should be reviewed and updated regularly to ensure they remain relevant and accurate.
- Utilize Electronic Health Records (EHRs): Many EHR systems offer built-in templates and features to streamline documentation.
The Role of Technology in Documentation
Technology is increasingly playing a significant role in physical therapy documentation. Mobile apps and electronic health record systems allow therapists to capture and store patient data quickly and efficiently. These tools can also facilitate communication and collaboration among healthcare providers. However, it’s crucial to ensure that any technology used is secure and compliant with HIPAA regulations.
Importance of Quality Control
Regular quality control checks are essential to ensure the accuracy and completeness of documentation. This can involve peer review, checklists, and audits. Implementing a system for tracking and correcting errors can significantly improve the quality of documentation.
Conclusion
Effective physical therapy documentation is a cornerstone of patient care. By utilizing well-structured templates, incorporating detailed observations, and prioritizing clear communication, therapists can ensure that patients receive the best possible care. Physical Therapy Documentation Templates are a valuable tool, but their effectiveness depends on consistent application and a commitment to quality. Ultimately, accurate and comprehensive documentation empowers patients, informs treatment decisions, and contributes to improved outcomes. The ability to accurately and comprehensively document a patient’s journey is a critical skill for any physical therapist.