The process of therapy can be complex and deeply personal. Effective communication between therapists and clients relies heavily on clear, concise, and well-organized documentation. A crucial element of this process is the use of a standardized therapy progress note template. This document serves as a record of the client’s progress, challenges, and treatment plan, facilitating continuity of care and providing valuable insights for the therapist. A thoughtfully designed template ensures that information is readily accessible and accurately reflects the client’s experience. Choosing the right template is paramount to ensuring the document’s effectiveness. This article will explore the importance of therapy progress note templates, different types available, best practices for their use, and how to tailor them to individual client needs. Understanding the nuances of these templates is vital for both therapists and clients seeking optimal therapeutic outcomes. Let’s delve into how to create and utilize a robust therapy progress note template.
The Importance of Standardized Documentation
The benefits of utilizing a standardized therapy progress note template extend far beyond simply recording information. It fosters accountability, improves communication, and ultimately contributes to a more consistent and effective therapeutic experience. Without a consistent format, therapists can struggle to accurately recall details, leading to potential gaps in the record and hindering the client’s progress. Furthermore, a standardized template ensures that all relevant information is captured, reducing the risk of miscommunication and ensuring that the client’s needs are consistently addressed. It’s a foundational element of ethical and professional practice. The ability to quickly and easily access a complete history of a client’s engagement is invaluable, particularly in cases where multiple therapists are involved or when the client’s needs evolve over time. Ultimately, a well-structured progress note template streamlines the therapeutic process, allowing therapists to focus on building rapport and facilitating meaningful change.

Types of Therapy Progress Note Templates
Several variations of therapy progress note templates exist, each designed to suit different therapeutic approaches and client needs. Some common types include:
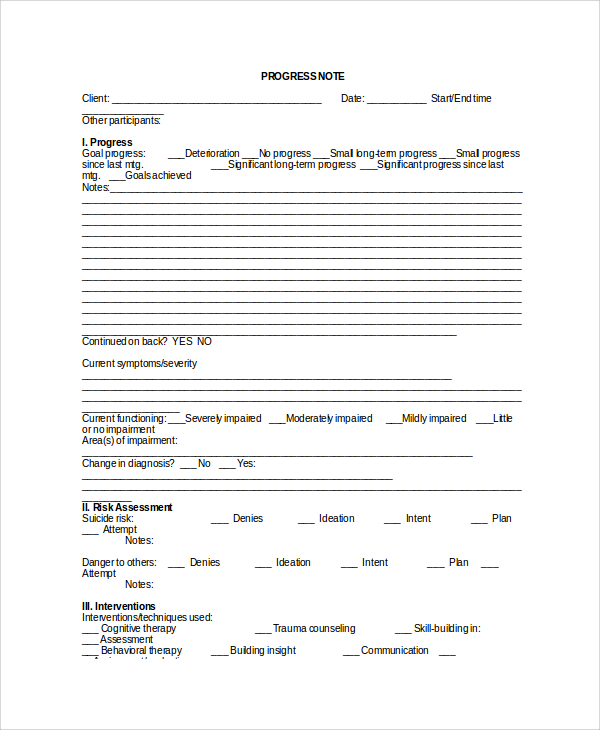
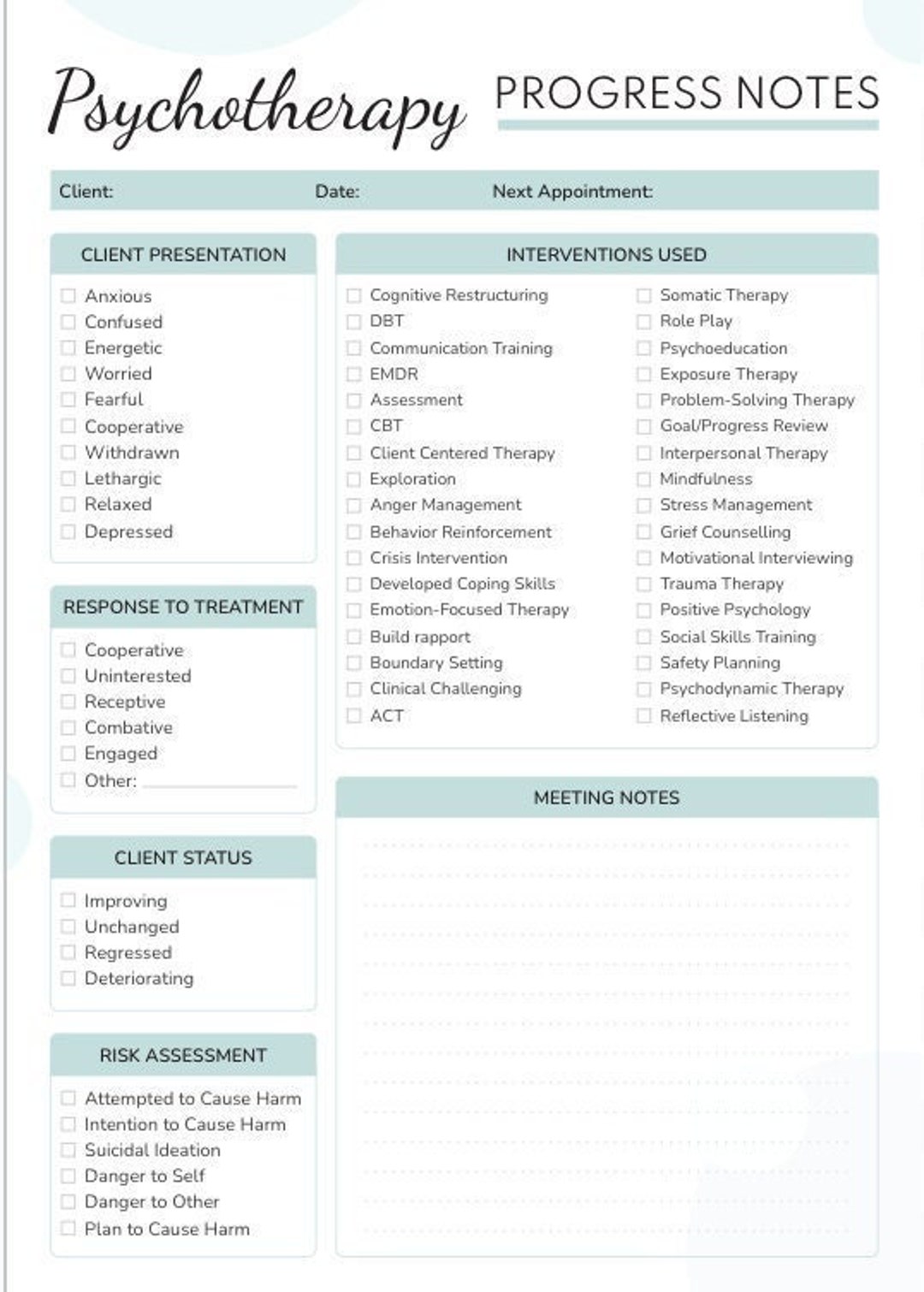
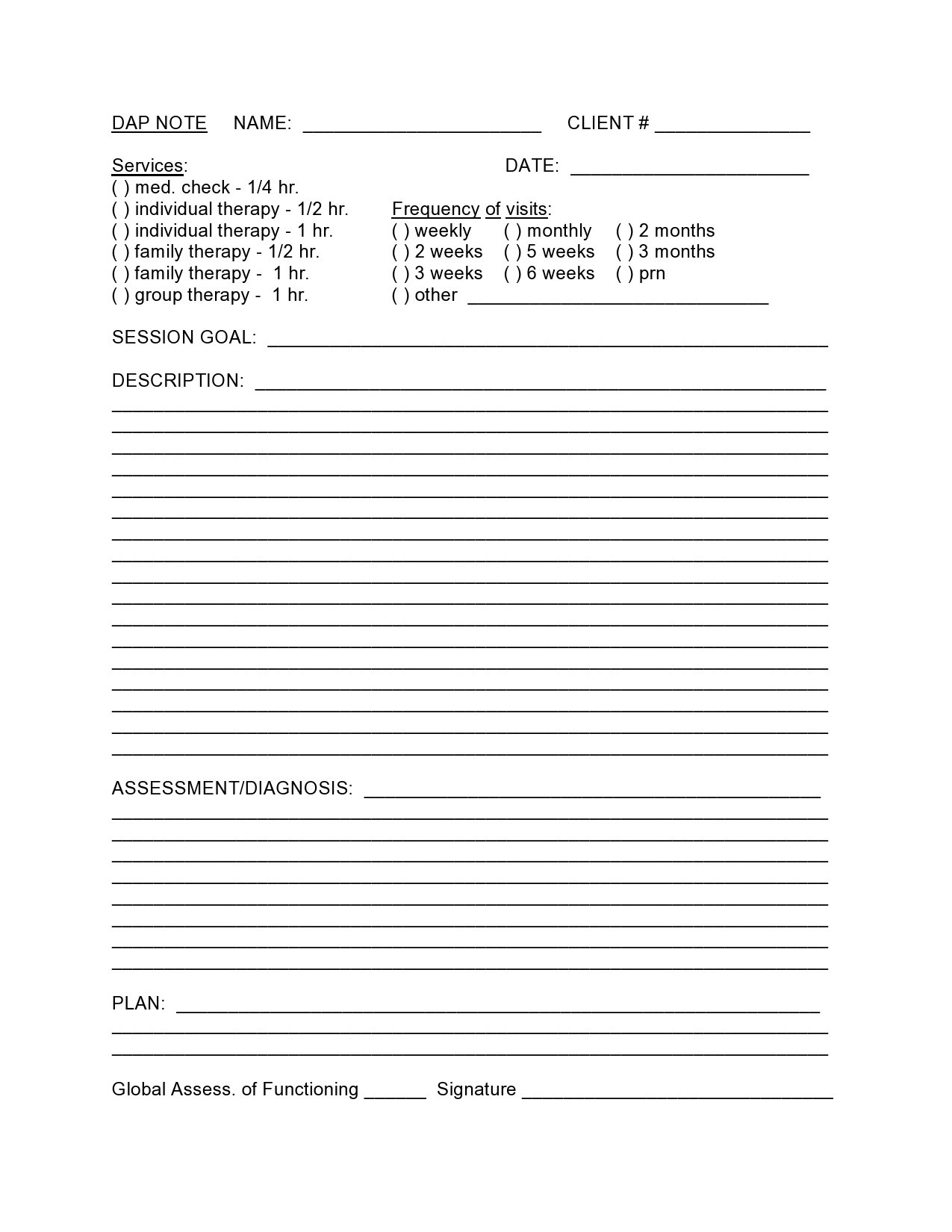
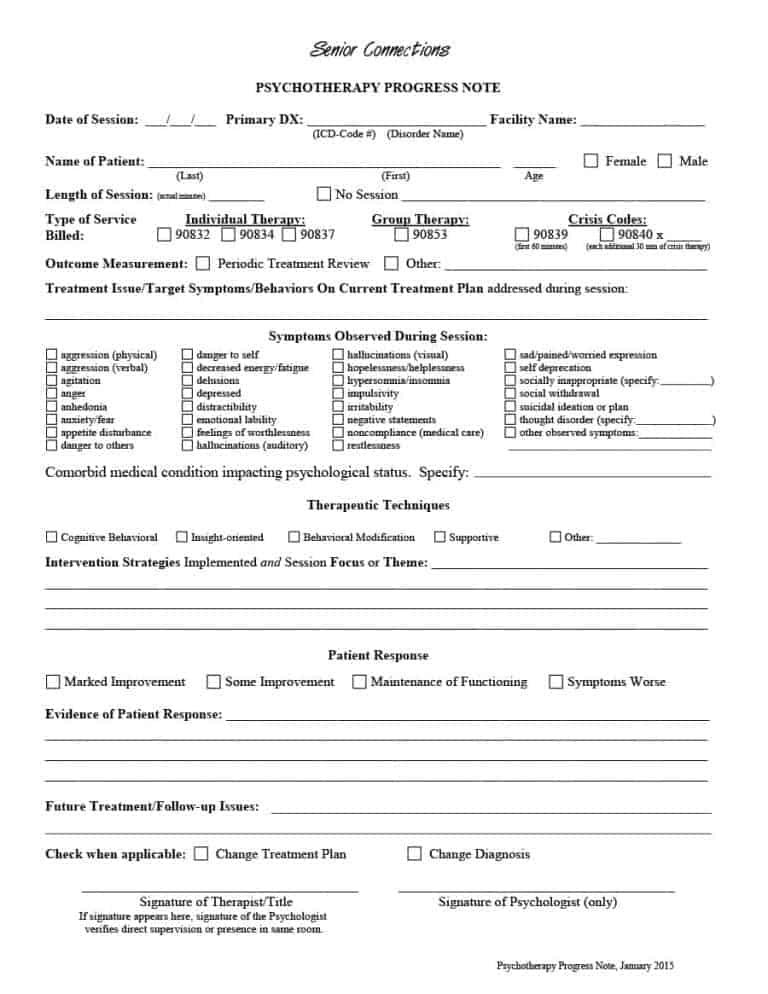
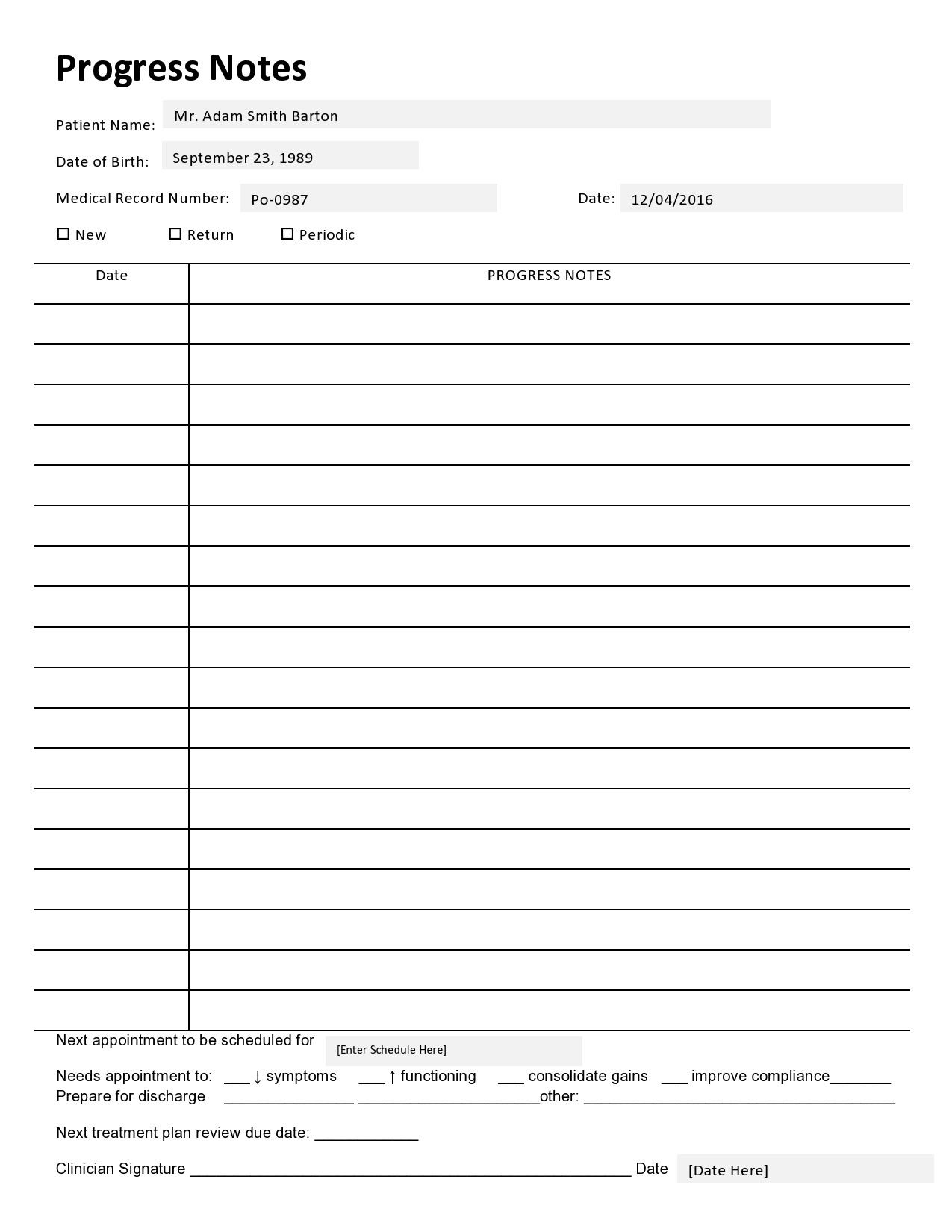
- Traditional Template: This is the most common type, featuring a structured format with sections for demographics, assessment data, treatment goals, progress summaries, challenges, and next steps. It’s a versatile option suitable for a wide range of therapeutic modalities.
- Cognitive Behavioral Therapy (CBT) Template: Specifically tailored for CBT, this template emphasizes identifying and challenging negative thought patterns and behaviors. It often includes sections on thought records, behavioral observations, and relapse triggers.
- Solution-Focused Therapy Template: This template focuses on identifying and building on the client’s strengths and solutions. It emphasizes exploring past successes and identifying potential pathways to future growth.
- Trauma-Informed Template: This template incorporates specific considerations for trauma survivors, including assessment of trauma history, safety planning, and addressing potential triggers. It often includes sections on coping mechanisms and emotional regulation.
- Digital Progress Note Templates: Increasingly popular, these templates utilize electronic platforms for secure and efficient record-keeping. They often include integrated forms and automated reminders.
Choosing the appropriate template depends on the specific therapeutic approach employed and the individual client’s needs. It’s crucial to select a template that aligns with the therapist’s expertise and the client’s preferences.
Key Sections of a Therapy Progress Note Template
Let’s examine some of the essential sections commonly found within a therapy progress note template. Each section plays a vital role in providing a comprehensive overview of the client’s progress.
1. Client Demographics & Contact Information
This section provides basic information about the client, including their name, date of birth, contact information (phone number, email), and insurance information. It’s essential for maintaining accurate records and facilitating communication.
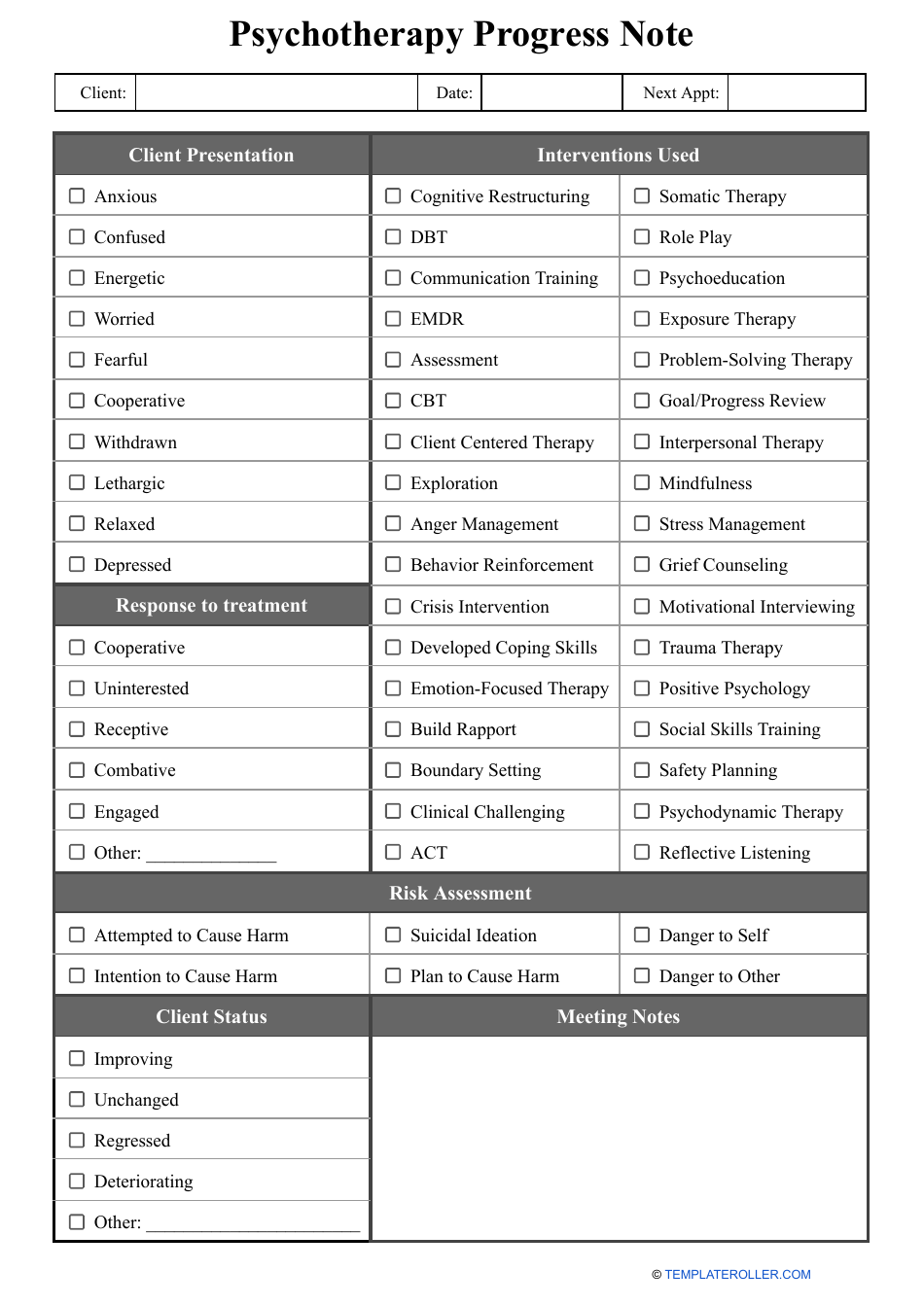
2. Initial Assessment & Goals
This section summarizes the initial assessment conducted, including the client’s presenting problems, strengths, and areas of concern. It also clearly outlines the client’s initial goals and therapeutic objectives. This section is particularly important for tracking progress towards established goals.
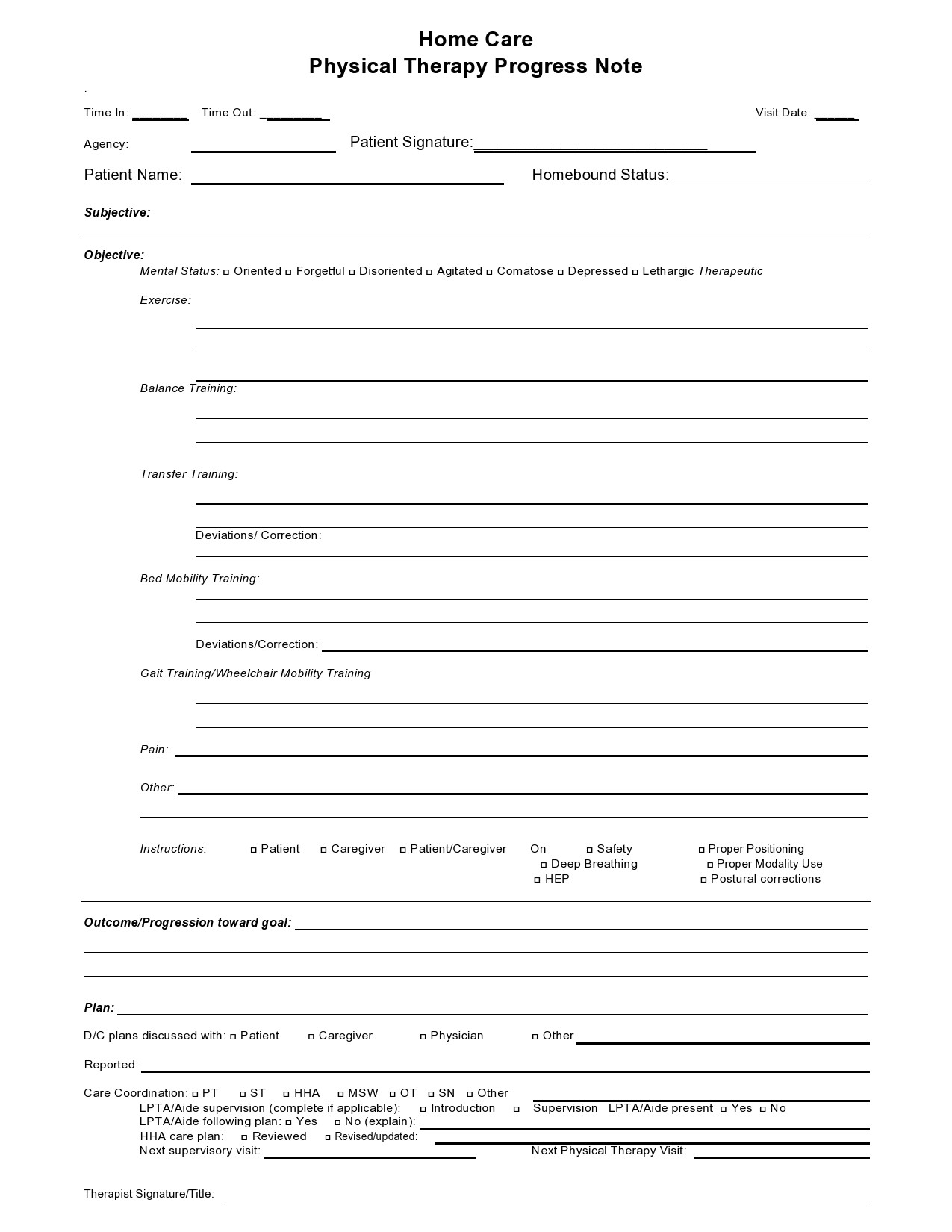
3. Treatment Progress – Summary
This is the core of the template, detailing the client’s progress towards their goals. It should include:
- Treatment Activities: A chronological list of all interventions delivered, including the date, duration, and description of each activity (e.g., individual therapy sessions, group therapy, medication management).
- Client’s Reported Feelings & Experiences: A space for the client to describe their emotional state, any changes in their thinking or behavior, and any concerns they have. This provides valuable insight into the client’s subjective experience.
- Progress Towards Goals: A clear statement of whether the client is making progress towards their stated goals. Quantifiable data (e.g., “Client reported a decrease in anxiety symptoms”) is highly beneficial.
4. Challenges & Obstacles
This section identifies any challenges or obstacles the client is facing, and how they are being addressed. It’s crucial to acknowledge difficulties and collaboratively develop strategies for overcoming them.

5. Safety & Well-being
This section addresses any safety concerns the client may have expressed, and any strategies being implemented to promote their well-being. It’s vital to ensure the client feels supported and safe.
6. Next Steps & Plan
This section outlines the next steps in the therapeutic process, including any planned interventions, follow-up appointments, and resources to be provided. It should be realistic and achievable.
Best Practices for Using Therapy Progress Note Templates
Effective utilization of a therapy progress note template requires adherence to several best practices.
- Be Concise and Focused: Avoid unnecessary detail. Focus on the most relevant information.
- Use Clear and Precise Language: Avoid jargon and ambiguous terms.
- Maintain Objectivity: Present information objectively, without personal opinions or judgments.
- Regularly Review and Update: Review and update the template periodically to ensure it remains relevant and effective.
- Collaborate with the Client: Involve the client in the creation and review of the template to ensure it meets their needs.
- Document Everything: Even seemingly minor details can be valuable information.
The Role of Technology in Therapy Progress Note Templates
The rise of electronic health records (EHRs) and digital progress note templates offers significant advantages. These platforms streamline the process of documentation, improve accessibility, and enhance data security. However, it’s crucial to ensure that digital templates are secure and compliant with privacy regulations. Furthermore, therapists should be trained on how to effectively utilize these tools.
Conclusion
Therapy progress note templates are an indispensable tool for therapists and clients alike. By utilizing a standardized format, documenting progress effectively, and addressing potential challenges, therapists can foster a more effective and collaborative therapeutic relationship. A well-designed template, coupled with best practices for utilization, can significantly enhance the quality of care and contribute to positive outcomes. Remember, the template is a tool to facilitate communication, not a rigid set of rules. Adaptability and a focus on the client’s unique needs are key to maximizing its benefits. Ultimately, a thoughtfully crafted progress note template empowers therapists to provide the best possible care.